
19 Jan Emboli detection and differentiation for stroke risk evaluation
HITS (High Intensity Transient Signals) Detection for Stroke Management
Because of missing collateralisation beyond the Circle of Willis, occlusions of cerebral arteries result in hypoperfusion or according to size and localisation of the embolus in stroke.
Different studies concordantly show that emboli detection is an adequate technical method to narrow the probability of embolic aetiology of stroke [Lund C. et al., 2000; Grosset D.G. et al., 1994].
Generally, in terms of pathophysiology, two different types of emboli should be distinguished: solid (e.g. plaque material) and gasous (e.g. air embolism).
According to size, origin and count, emboli do have different clinical relevance. Whereas small amounts of air embolism can be reabsorbed and metabolised within brain capillaries before hypoperfusion or even stroke occurs, solid emboli (e.g. plaque material scattered during carotid stenting) are resorbed or broken down significantly slower.
Physical background
Whereas measurement of blood flow velocity by change of reflected Doppler frequency belongs to clinical routine in most hospitals, change of received Doppler intensity is important to detect embolic signals.
Such intensity modulations result from US reflections at interfacial tissues with different acoustic impedances (e.g. between air and blood), which can be detected by ultrasound sensitively. Typically, short, high-frequent signals (HITS) can be derived, which are not easy to distinguish from artefacts. Doppler justification should consider a low gain amplitude and a small sample volume to reduce mismeasurement.
Literature references to reduce gain as far as possible that HITS impress more obviously within the pattern, which therefore reduces rate of nonobservence.
Emboli Detection
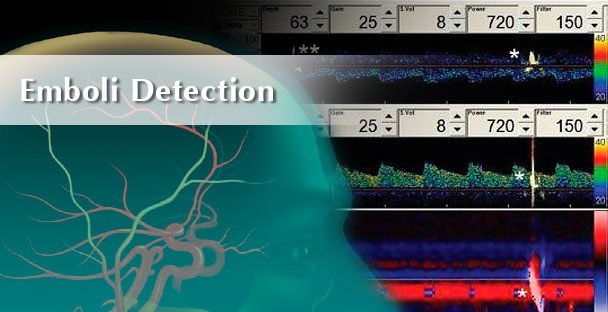
Emboli detection using transcranial Doppler ultrasound is based on HITS detection. Microembolic signals (MES) are brief, high-intensity transient signals (HITS) that occur when microemboli pass through the ultrasound beam. HITS are short, overshooting Doppler patterns. In contrast to artefacts, HITS generate solely unidirectional signals.

Identification of HITS should be based on the guidelines of “Consensus Committee of the Ninth International Cerebral Hemodynamic Symposium“, 1995:
- A Doppler microembolic signal is transient, usually lasting less than 300 milliseconds. Its duration depends on its time of passage through the Doppler sample volume.
- The amplitude of a Doppler microembolic signal is usually at least 3 dB higher than that of the background blood flow signal and depends on the characteristics of the individual microembolus.
- Within the appropriate dynamic range of bidirectional Doppler equipment, a signal is unidirectional within the Doppler velocity spectrum.
- The maximum of the signal belongs to the envelope courve.
- Depending on the equipment used and its own velocity, a microembolic signal is accompanied by a “snap,” “chirp,” or “moan” on the audible output.
Modified from: Dissertationsschrift von Alexandra Schröder, Rhein-Ruhr-Universität Bochum, 2004
Emboli Differentiation
In Monitoring with automatic Emboli Detection, emboli can also be differentiated between solide and gaseous. Microembolic signals (MES) are brief, high-intensity transient signals (HITS) that occur when particulate micro emboli or gaseous microbubbles pass through the ultrasound beam. HITS are short, overshooting Doppler patterns. In contrast to artefacts, HITS generate solely unidirectional signals.